
Effect of Miotic/Mydriatic Agents on Eye and Molecular Mechanism
Tweet
Eye: By Bishnu Marasini
Eye maintains the proper visualization and clear image by controlling influx of light by smooth muscles that control the size of the pupil and the degree of adjustment is controlled by autonomic nervous system. These muscles are radial muscle of the iris (dilator papillae) (Iris dilator/radial muscle) and the circular muscle of the iris (constrictor papillae) (iris circular/sphincter muscle).
Iris dilator/radial muscle is arranged radially in the iris and therefore fit as a dilator. It is innervated by the sympathetic system, which acts by releasing noradrenaline, which acts on α1-receptors. Its action to dilate lens let more light to reach in retina. Iris sphincter/circular muscle encircles the eye and constricts the lens. It is controlled by parasympathetic fibers that originate from the Edinger-Westphal nucleus, travel along the oculomotor nerve (CN III) through the superior orbital fissure and synapse in the ciliary ganglion, and then the postganglionic PSN fibers leave enter the eye via the short ciliary nerves. Acetylcholine is the transmitter of signal to it. The lens of the eye is attached to the cillary body by suspensory ligaments. When the circular/sphincter muscle is relaxed, the cillary body exerts tension on the lens causing it to flatten (for far vision). When the Circular/sphincter contracted; then lateral tension on the lens decreases and thickens (for near vision; cycloplegia). Circular and radial muscle act on the “tug of war” fashion; one is contracted other will relaxes.
Mydriasis and Miosis:
“Mydriasis" is an excessive dilation of the pupil due to disease, trauma or the use of drugs. “Miosis” is constriction (or excessive, sometime abnormal) of the pupil of the eye.
Mydriasis is mainly caused by the agents which are muscarinic (M3) antagonists (indirect) and adrenoreceptor (α1/α2) agonists (direct). Similarly miosis is caused by the agents which are muscarinic (M3) agonists (direct) and adrenoreceptor (α1/α2) antagonists (indirect). Also, cAMP inhibiting agents also reduce the degree of contraction of these muscles by decreasing Ca++ level in muscle by hyperpolarization. In addition to this; miotic/mydriatic agents might be systematically acting (administered in the part of body other than eye) or locally/topical acting (administered in the eye).
Miotic agents: dappiprazole (α1-antagonist), pilocarpine (M3 agonist), isoproterenol, thromboxane A2, yohimbine, Tolazoline, prostaglandin growth factor 2α (PGF2α), inomysin, thapsigargin etc.
Mydriatic agents: clonidine and tizanidine (α2 agonist), methoxamine (α1-agonist), phentolamine, Phenoxybenzamine, 8-chloroethylamine and phenylephrine (α1L-AR agonist), cyclopentalate and atropine (M3 antagonist), moxonidine, guanabenz etc.
Mechanism:
Pilocarpine increase the degree of contraction of sphincter muscle cell by activating Gq/11 signaling linked to M3 receptor. Atropine blocks activity of M3 agonist competitively binding on the receptor and sphincter muscle could not contract and dilator muscle vanquish on contraction as in tug of war fashion resulting mydriasis.
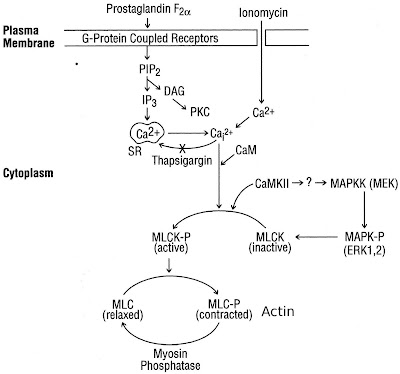
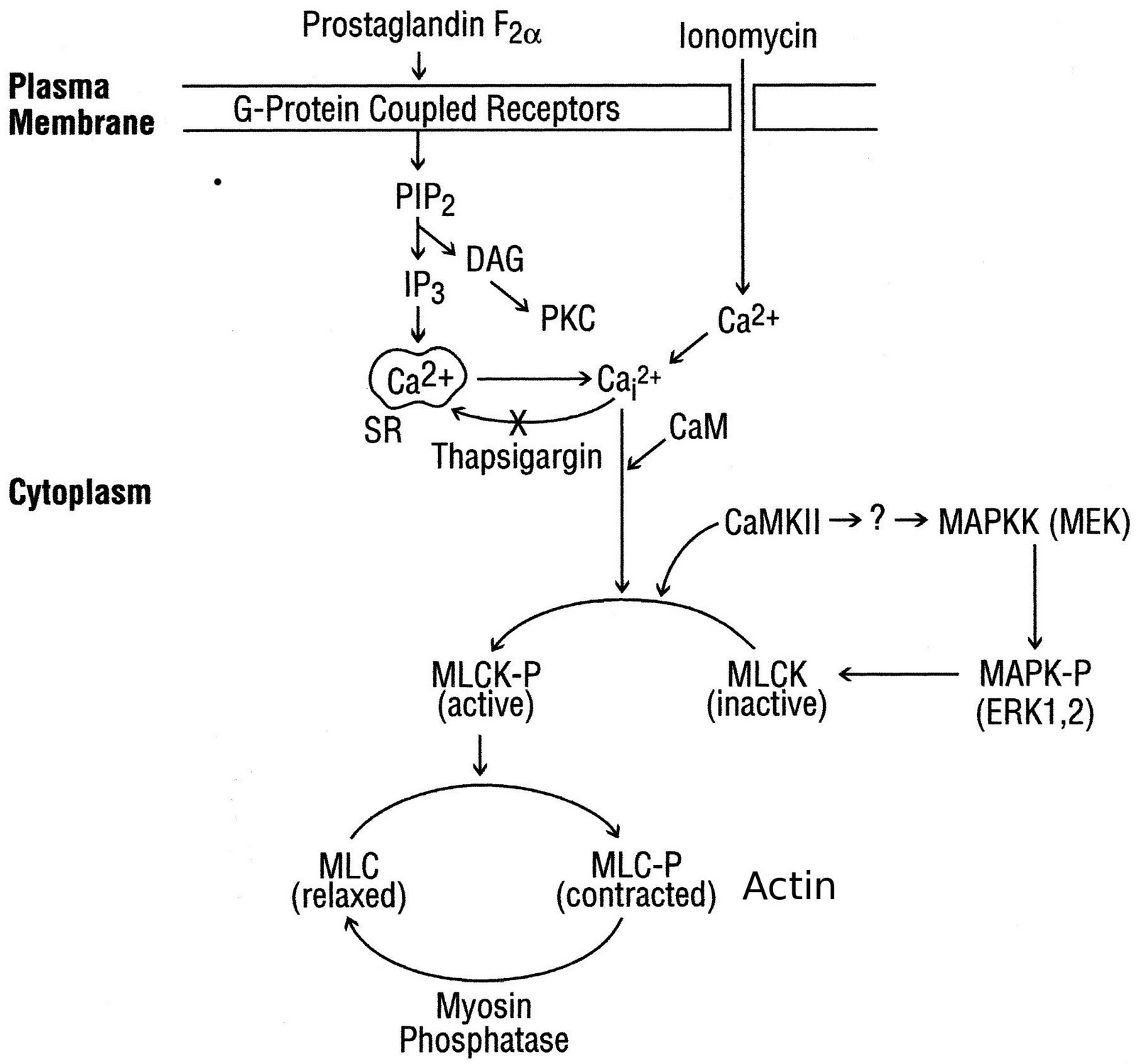
Iris sphincter muscle cells express M3 receptor on their surface which is linked with pertussis toxin-insensitive G protein Gq/11, resulting in hydrolysis of membrane phospholipids; subsequent activation of phospholipase C-b (PLC-b) generates the major second messengers inositol (1,4,5)-trisphosphate (IP3) and diacylglycerol (DAG). Inositol(1,4,5)-trisphosphate binding to its receptor on intracellular storage sites results in mobilization/increasing cytosolic Ca2+ from extra cellular source and/or golgi bodies. Then Ca++ becomes available into the sarcoplasm and binds to troponin molecules in the thin filaments causing the troponoin to change the shape. This change in shape releases the troponin-tropomyosin complex from the myosin binding sites on the action. Contraction power strokes use ATP; myosin heads bind to actin, swivel and release; thin filaments are pulled toward center of sarcomere and finally contraction of the muscle. The increased Ca2+ in cytosol activates different mechanism/pathways; in which it actives rapid phosphorylation and activates of p42/p44 mitogen-activated Protein Kinase (MAPK), Ca2+/calmodulin-dependent protein kinase II (CaMKII) and myosin light chain kinase (MLCK), and other signaling cascade activating other enzymes as well as phosphorylation of myosin light chain (MLC) phosphorylation and contraction.
The miotic and mydriatic effect also found by nonadrenergic, noncholinergic response of the iris has been found in recent years in neurotransmitter binding site e.g., neurokinin A and B (NKA, NKB) which influx Ca2+ but not through the voltage-dependent channels, which are opened on depolarization of the membrane, mainly through the L and N types.
The Ca2+ channels and the signalling pathways activated by ET-1 in the isolated rabbit iris sphincter. A scheme showing the signalling pathway activated by ET-1 to elevate [Ca2+]i and induce contraction is given below: We show that contraction of the iris sphincter by ET-1 or carbachol depends on the influx of extracellular Ca2+, as shown by abolition of the contraction after removal of extracellular Ca2+ nifedipine had minimal effects on the ET-1-induced functional responses. This latter observation is interesting because in cat iris sphincter, the Ca2+ mobilizing agonists PGF2α, ionomycin and thapsigargin increased MAP kinase phosphorylation and contraction.
In the eye, the activation of EP1, EP4, and FP receptors by their selective agonists reduces intraocular pressure and causes pupil constriction.
11
comments
![]() Labels:
Article,
Biology,
Molecular-biology
Labels:
Article,
Biology,
Molecular-biology
